Although a growing number of antibody–drug conjugates (ADCs) have been approved as cancer therapeutics, the full promise of ADCs has yet to be fully realized, owing to issues with stability and the resulting toxic side effects. In this Q&A, Philipp Spycher, Ph.D., Chief Executive Officer and founder of Araris Biotech, discusses his company’s new peptide linker technology, which has been shown in preclinical studies to enable highly targeted delivery of payloads with minimal loss during circulation, with Pharma’s Almanac Editor in Chief David Alvaro, Ph.D.
David Alvaro (DA): Can you start the discussion off with a concise historical overview of Araris Biotech, particularly how the company has evolved over the few years since we last featured you in Pharma’s Almanac?
Philipp Spycher (PS): I incorporated the company at the end of January 2019 after I completed my postdoctoral studies. My vision was to cure cancer with antibody–drug conjugates (ADCs). It was a big vision and is still the same vision, but during our journey over the last three and a half years, we achieved several milestones. We raised a significant financing round in October of 2020 with mainly UK- and Swiss-based investors, built out the team with additional experts from various fields, expanded the advisory board, and significantly grew and strengthened the company overall.
On the technology side, we have also further evolved the company to the point where we believe that we are getting close to realizing that vision. The more data that come out from the lab, the more excited the team and everybody gets, especially since the data is highly consistent. The vision was to generate a technology that enables us to deliver on the promise of site-specific ADCs and their expansion of the therapeutic index. By doing so, it would mean that we can go for targets and indications not possible with conventional ADCs and thus expand on their applications and deliver on the promise of curing cancer.
DA: How would you characterize the present moment in the overall trajectory of the ADC sector?
PS: There has been significant evolution in the ADC space accompanied by real learning. The key focus now is on the ability to design effective ADCs with a high therapeutic index, particularly having stable payload attachment on the antibody and selecting the right payload — not necessarily the most potent ones. We have seen that less potent payloads can actually help deliver compelling data, and those successes have triggered more interest in the ADC space. People now really appreciate the ability of ADCs to deliver toxins to the tumors and kill them.
Recent clinical data have been unbelievable showing that applying new linkers and payloads can make a huge difference. There are great opportunities for Araris, because we can generate really stable ADCs directly from ‘off-the-shelf’ antibodies and virtually hook up any payload there is in a very simple and efficient way. In general, renewed interest in ADCs was triggered by the numerous acquisitions of small biotechs, such as VelosBio by Merck and NBE Therapeutics by Boehringer Ingelheim, as well as Immunomedics by Gilead and the licensing deal between Daiichi Sankyo and AstraZeneca.
DA: With respect to addressing some of those key challenges, such as stability, heterogeneity, and development timelines and costs, what general solutions are in play in the industry, and, more specifically, what approach has Araris taken?
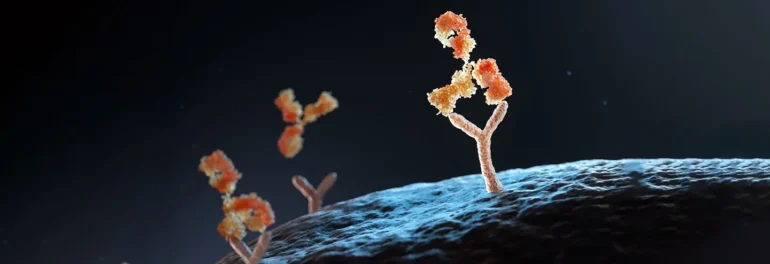
PS: Addressing the stability of the overall molecule and how to efficiently deliver high amounts of payloads to the tumor are still the key issues. It is also crucial to ensure that attaching a payload to an antibody does not affect the properties of the antibody or the payload release. Conventional ADCs suffered because the properties of the antibodies were altered once the payload molecules were attached, which limited their ability to deliver the cytotoxic compound to the target tumors. Additionally, when the payload isn’t stably attached to the antibody, it can be released too early, leading to side effects and a lower therapeutic index as well. Those issues were very common.
With the technology that we have developed at Araris Biotech, we can generate stable ADCs that have pharmacokinetic (PK) profiles similar to the antibody; they provide high exposure of the cytotoxic agent to the tumor tissue. We have data showing high activity at low doses combined with high tolerability, and, as a result, our candidates have significantly higher therapeutic indices compared with conventional ADCs.
DA: Can you elaborate on what is unique about Araris’ linker technology and how it enables those benefits?
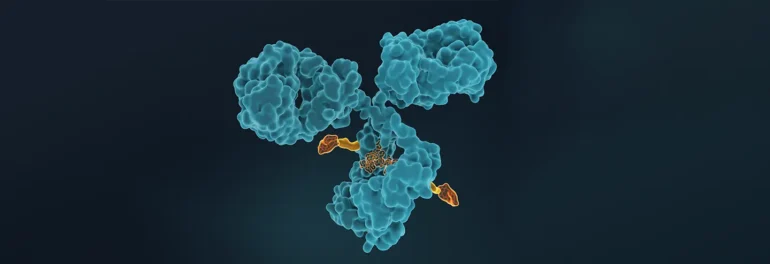
PS: There are multiple aspects to our technology, but what is really key is that the payload is attached to a privileged attachment site on the antibody so that the pharmacokinetic profile of the resulting ADC is essentially identical to the unmodified antibody. That enables the delivery of high amounts of payload to the tumors. Also important is the design of the linker to ensure that the payload is stably attached to the antibody while traveling to the tumor but then is released specifically at the targeted site. With our technology, once the ADC is internalized into the tumor cell, the degradation of the linker happens very efficiently.
The reason we can achieve such behavior is because we use hydrophilic peptides as linkers. They enable site-specific conjugation and efficient release of the payload within the target cell. In addition, this approach ensures biocompatibility, which we think is a critical factor that has mostly been overlooked. There is a particular enzyme in the body that may be involved in neutropenia, a dose-limiting toxicity for many ADCs. The enzyme thereby recognizes certain sequences in the linkers, causing its cleavage and thus loss of the payload, eventually killing neutrophils.
With Araris’ technology, we have data showing that we have significantly reduced neutropenia compared with other ADCs. We can achieve this performance because we have optimized the linkers so that they are not cleaved by this enzyme but are metabolized at the target site and result in the release of the payload. We believe that our ability to design such stable linkers that enable efficient release only at the targeted site is unique in the entire ADC space.
DA: What impact does your technology have on the manufacturability of ADCs?
PS: We have made a lot of progress on the manufacturing side. Payload attachment used to require multiple steps, but today we have reduced that down to just one. In addition, we don’t need to do any engineering of the antibody to prepare it for use as an ADC. We can work with off-the-shelf antibodies and attach payloads in a single step.
Another advance was a reduction in the amount of payload used. Earlier processes required the use of large excesses of the payloads, which are quite expensive, since they are complicated chemical compounds. Now, we only need to use a minimal quantity, which significantly reduces purification requirements and costs.
Finally, the linker we use is quite hydrophilic, and the location of the payload attachment is not as exposed as is typically the case for other conjugation sites, which in combination results in ADCs that have very good hydrophilicity — much better than that seen for conventional ADCs. Hydrophilicity is important for solubility and bioavailability.
DA: When we last spoke, Araris Biotech was pursuing a hybrid, two-pronged business model including both partnering and in-house development of your own ADCs. How has your internal pipeline evolved?
PS: We have made a lot of progress developing our own ADC assets in liquid and solid tumor types. Our lead product is an anti-CD79b ADC now in preclinical development. The discovery phase for this molecule has been completed, and we hope to advance into clinical development by early 2024. It is a very exciting candidate, because we think we can go into an indication that has previously not been possible for conventional ADCs.
A second program is underway that aims to go for solid tumor targets with a focus on difficult-to-treat solid tumor indications, which makes it especially exciting.
DA: When it comes to partnerships, are you looking for specific types of companies or are you more agnostic to whatever is possible?
PS: We are open to partnering with any pharma companies that are looking to develop effective ADC-based therapies. Our goal is to enter into high-value partnerships.
In that regard, we are seeing significant interest, because ADCs are a very hot topic at the moment, and we think that creating stable linkers is the crucial element for achieving success. The ability to attach multiple payloads on the same antibody is also of real interest. Araris Biotech’s linker technology can address both issues — including the attachment of up to four of the same or different payloads — and we are discussing this with many different pharma companies.
DA: Is that something that has been possible before — linking multiple payloads to a single antibody?
PS: When we talk to people in the field, it seems that everyone is working on developing a solution, but only very few have yet published any data demonstrating a real benefit. It is early right now, but I do think that in the next few years we will see very exciting progress published.
I am very excited about this development of attaching more than just one type of payload on the antibody. I think it really offers a completely new avenue for ADC design. Araris Biotech is very well positioned, because we can chemically control the attachment of the payload nicely, and we can create such ADCs quite easily.
DA: Is there anything else that you’d like to share about how the company has evolved over the last couple of years in terms of investors, funding, or expansion of the team?
PS: We started as a spin-off company from the Paul Scherrer Institute (PSI) and ETH Zurich and are presently still located at the original incubator site in Zurich. But Araris Biotech has matured sufficiently, and we are excited to be moving during the summer to a new location and becoming fully independent. Our team now comprises 10 people, and we will soon be hiring additional members. Growth in that regard will continue over the months and years to come. In addition, our advisory board has been expanded to include experts with experience designing clinical trials and supporting target identification.
In terms of financing, we are currently active with Series A fundraising. It is very good to be in the ADC space, but we are seeing lots of interest in our technology in particular because of the exciting data that we have generated thus far. For instance, our lead molecule has shown remarkable tolerability in monkeys where conventional ADCs would have shown significant toxicities or even deaths.
DA: How do you anticipate the ADC sector evolving further over the next few years? Are any big developments expected? And what contribution do you think Araris will make to that evolution?
PS: Our vision is to provide a functional cure for some cancers. If we can show in clinical development that the compelling preclinical tolerability results in monkeys and activity results in mice translate well into humans, I think we could potentially set the new benchmark in ADC linker technology. The overall result should be a significant improvement in the therapeutic index that would really enable us to deliver on the promise of site-specific ADC technology. We should be able to expand into indications or applications that have previously not been possible with conventional ADCs.
That is the key focus: improving the therapeutic index. But doing so has traditionally been very challenging, because the payloads are lost while the ADCs are in circulation. If the linker-payload is too exposed, the linker may be cleaved prematurely or the ADC may have an altered PK-profile, leading to decreased toxin delivery to the tumor and a narrow therapeutic index. With the Araris linker technology, we believe that we can achieve an improvement in the therapeutic index because of the greater stability, unchanged PK-profile, and cleavage mechanism of our linkers.
For this reason, I hope that with the technology we will make a real impact on treating cancer patients. At Araris, the whole team, as well as our scientific advisory and investor board members, also share this vision.
As with all novel pharmaceutical technologies, the effectiveness of the technology will be shown in the clinic. I think that Araris Biotech has every reason to believe that the molecules that we are developing with our new ADC linker technology are very strong candidates that will be safe and efficacious and have good therapeutic indexes.
Originally published on PharmasAlmanac.com on July 7, 2022.
Theranostics — Radioimmunoconjugates that can be used in both diagnosis and therapy — show significant promise for complementing and supplementing immunotherapies as personalized cancer treatments. As theranostics are high-value and complex products comprising vectors, linkers, and payloads, specialized expertise in bioconjugation is essential to the development and manufacture of optimal candidates that can provide highly targeted diagnostic and therapeutic benefits. GBI has extensive experience helping clients rapidly bring safe and effective theranostic products to the market.
The Nature of Theranostics for Cancer
Theranostics is derived from the words therapeutics and diagnostics. A patient receiving theranostic treatment is simultaneously or sequentially diagnosed and treated using one or more drugs and/or techniques in a single “package.” By diagnosing and treating patients in one session, time and money are saved, and, in many cases, undesired side effects that occur when these steps are implemented separately can be avoided.1
For cancer patients, the combined use of diagnosis and therapy tools also enables a personalized approach to treatment.2 Typically, positron emission tomography (PET) imaging is used to determine whether specific tumor receptors are present on a patient’s cancer cells. If detected, a radioactive drug is delivered in a highly targeted manner to the cancer cells to destroy them without harming healthy cells.3
This targeted delivery is achieved by using a radioimmunoconjugate comprising an antibody covalently linked to (or chelating) a radioactive payload. The antibody is the delivery system that brings the radioisotope or radionuclide to the targeted disease tissue. The intensity of the PET scans indicates the level of the disease and the extent of treatment required.
The somatostatin receptor (SSTR2) on the tumor cell membrane is a common target.4 The radioactive diagnostic drug Ga-68 DOTATOC binds to this receptor, making any tumors present in the body visible and detectable on a PET scan. If tumors are detected, the patient can then be injected with a different radiopharmaceutical, such as lutetium-177 (Lu-177) or yttrium-90 (Y-90), bound to the same somatostatin analog peptide that binds to the SSTR2 receptors, allowing the drug to target and kill the tumor cells.
Figure 1. Standard theranostic design targeting the somatostatin receptor (SSTR2) on the tumor cell membrane. 4,12,13
Theranostic treatment regimens are designed specifically for each individual based on information gained using pharmacogenetic, proteomic, and biomarker profiling data, which ensures that the right drug is delivered to each patient at the correct time.5 Because they involve an “intimate connection of diagnosis and therapeutics” that draws diagnosis and therapy closer, theranostic protocols have the potential to provide better outcomes than traditional therapy approaches.
Initially, iodine 131 (I131) was widely used as a diagnostic and therapeutic agent. Most theranostic developers today, however, are moving away from radioactive iodine, which is a beta emitter, and pivoting to other options (such as alpha emitter and the use of an appropriate hetero-bifunctional linker that is covalently conjugated to the antibody and chelated to an appropriate radionuclide — see below), owing to the poor signal-to-noise ratio associated with I131. Furthermore, since I131 is directly conjugated to the antibody without using a linker, the drug-design possibilities are relatively limited.
Vast Market Potential
The field of theranostics grew out of the field of diagnostic imaging, according to Steven R. Deitcher, M.D., President, CEO, and Board Member of radiation therapeutic innovator Radimmune. The first step was the development of solutions for the targeted delivery of gamma-emitting radioisotopes for nuclear medicine imaging. This technology was then applied to the targeted delivery of beta-emitting radioisotopes to treat the same diseases. Today, theranostics includes the use of a single antibody to deliver both a diagnostic agent and a therapeutic anticancer agent to specific tumor cells. A typical goal in the field is to develop a single antibody that delivers a single radioisotope that can serve as the diagnostic and therapeutic agent.
The potential for the theranostics market directly reflects the significant unmet needs that remain with respect to cancer treatment. “With over 1.9 million new cases and over 600,000 cancer deaths predicted for 2022 in the United States alone, there is plenty of room for improvement,” Deitcher states. Advances in PET technology, the growing use of alpha emitters, and improved manufacturing processes are also contributing to the growth of the theranostics market.
The possible applications of theranostics are numerous and include visualization of biological processes or tumor biology in vivo, diagnosis and tumor staging, therapy planning, and treatment of specific tumors.6 Importantly, theranostics accelerates the translation of potential tumor targets from preclinical research into first-in-human clinical studies.
One challenge of some significance is the supply and sourcing of the raw radioisotopes used in the production of radionuclide payloads, particularly for alpha-therapeutics and theranostics. Fortunately, investments in new production capabilities are being undertaken to address this issue. What is needed, observes Deitcher, is more favorable data from robust clinical trials to drive patient and physician demand that would prompt production innovation and investment geared toward alleviating the current supply issues.
Despite the potential headwinds, the value of the global theranostics market is expected to maintain a compound annual growth rate (CAGR) of ~9.5–12.2% in the coming years, reaching $124–$153 billion by 2027/2028. 7,8
Moving from Diagnostics to Therapeutics
Many companies developing theranostic solutions start with a purely diagnostic product, typically a radioisotope conjugated to a specific antibody that can be used to determine whether a patient has cancer and the severity of the disease. Nearly in parallel, they develop a complementary therapeutic using a different antibody–chelated payload combination.
This approach enables the “assess it and treat it” concept while also allowing these companies to demonstrate the effectiveness of the antibody for targeting the tumor and time to raise money for the development of companion therapeutics.
Alpha, Beta, and Gamma Emitters
Radionuclides used as payloads in theranostic applications are either alpha-, beta-, or gamma-emitters. Alpha particles are essentially the nuclei of helium atoms (two protons and two neutrons), while beta particles are electrons, and gamma particles are photons.
A notable difference between beta and alpha particles, beyond size and charge, lies in their respective linear energy transfer (LET) properties, according to Deitcher. LET describes the rate at which energy is transferred per unit length of track. Beta particles are lower energy and travel farther than alpha particles; thus, alpha particles can have LETs that are hundreds of times higher than those of beta particles. That makes them attractive for therapeutic applications, because if delivered very close to the cancer cell nuclei, they can kill tumors while avoiding or minimizing collateral damage to healthy cells.
It is also worth noting, however, that the use of radioactive — and nonradioactive — payloads that have already been approved in other applications confers an advantage with respect to providing a level of comfort for patients, physicians, and regulatory authorities that the agent is known to work in a clinical setting and has well-characterized safety risks.
Theranostic Delivery Systems
Antibodies currently serve as the most widely used delivery systems for theranostic applications, and they are often biosimilars with demonstrated binding behaviors. Therefore, these radioconjugates represent a subtype of antibody–drug conjugates (ADCs). The specific nature of the disease will dictate the optimum delivery vehicle, linker, and payload.
While antibodies effectively target specific cell receptors, their use has some limitations. For instance, different cancers at different stages in different groups of patients may require different delivery vectors, according to Deitcher. Tumor affinity, tumor selectivity, the pharmacokinetics of the vector and the chosen radioisotope, clinical activity, and safety must all be considered.
Non-antibody delivery vectors can be attractive, because it is much easier to quickly screen large numbers of them. Examples include peptides, small molecules, and nanoscale systems. Peptides and small molecules,9 in theory, are easier to make and penetrate tumors more quickly than full-sized antibodies, but they are cleared from the body more quickly.
Nanoscale formulations can be derived from liposomes, dendrimers, polymeric nanoparticles, metallic nanoparticles, silica nanoparticles, magnetic nanoparticles, quantum dots, carbon nanotubes, polymeric micelles, scFV fragments and nanobodies (from camelids), among others.1,4,10 More recently, bacteriophages have attracted attention as possible drug-delivery systems. Because they are so small, nanoscale theranostics have the advantage of enabling the detection of tumors less than 0.5 cm in size.11 They also make it possible to prepare biomimetic materials.10 Challenges to their use include difficulty in producing particles that are uniform in size and highly reproducible, particularly when scaling up processes.11
Choosing the Right Chelator
It is not only important to choose the right vector and payload, but also the right linker or chelator. In addition to the necessary linkage chemistry for given vectors and payloads, it is also essential to consider whether the product will be used for diagnostic or therapeutic purposes. For diagnostic applications, the radionuclide must remain bound to the chelator, while for therapeutics, the chelator must release the payload at the target site.
To date, there have only been a limited number of commercially available chelators for use in theranostic applications, including cyclic 1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA), [(R)-2-Amino-3-(4-isothiocyanatophenyl)propyl]-trans-(S,S)-cyclohexane-1,2-diamine-pentaacetic acid (acyclic “CHX-A” linkers), TCMC (also known as DOTAM), and deferoxamine (DFO). DOTA is commonly used to produce diagnostic products, while CHX-A is used for therapeutics.
It is crucial for theranostic developers not to consider the linker to be less important than the delivery vehicle and the payload. While it may be the least expensive of the three components, it is equally important. It provides the means by which the payload is attached to the vector, without which there is no product. It also controls the release of the payload, which directly impacts therapeutic performance.
It should also be noted that not all isotopes require a linker; some can be directly bound to the vector.17,18, In addition, some linkers can only bind to a limited number of isotopes, while others work with a wide range of different types of isotopes, such that the same vector with one particular linker could be used to bind a diagnostic isotope or a therapeutic isotope. In this case, the same antibody–linker product could be used to support the diagnostic imaging and the therapeutics, with only the payload needing to be changed.
Fighting Melanoma with Theranostics
Radimmune was originally formed in 2016 with a primary focus of developing a universal targeted alpha-therapeutic for all subtypes of melanoma. The technology involves engineering an antibody that binds to extracellular accumulations of melanin (an intracellular molecule), unlike other companies in the field that are targeting cancer cell surface antigens or receptors. In addition, the company is looking to add to their pipeline and is considering some cell surface targets.
Melanin is a common feature of all types and cases of melanoma, whether cutaneous, uveal, mucosal, or acral melanoma. Melanin is not a protein but a pigment that is very difficult to bind. Radimmune’s anti-melanin antibodies bring isotopes into the tumor, and it is believed, according to Deitcher, that the antibodies bind to melanin that has leaked out of a few dead melanoma cells. The goal is to bind to that melanin and kill more melanoma cells, which further enriches the target tool.
Radimmune’s engineered humanized antibodies against melanin linked with several different alpha-emitters have been tested in animals using different tumor models. The company has generated some promising data and continue to assess opportunities for further optimization.
According to Deitcher, the company will continue to concentrate on some of the hardest-to-treat cancers and look for additional targets and opportunities that will hopefully make a difference in the lives of people with cancer.
Development and Manufacturing Challenges for Theranostics
The potential combinations of vectors, linkers, and payloads afford theranostic developers significant flexibility and numerous options for finding optimum solutions but also create challenges for development. There are many different permutations and combinations that must be evaluated. It can also be challenging, because access to proper imaging devices during preclinical and clinical development is essential.
With respect to manufacturing, the chemistry is fairly straightforward in most instances. The chelator is a heterobifunctional crosslinking reagent with reactive and metal-chelating groups at each end that selectively react with the antibody (or another vector) and chelate to the payload. The challenges derive more from the fact that the payload is a radioactive metal compound. It is critical to ensure that no metal contaminants, particularly heavy and transition metals, are present that could potentially bind to the chelator. Buffers and other reagents must be de-metalized before use, typically using a complexing agent, such as ethylene-diamine-tetra-acetic acid (EDTA) or metal-chelating resin column. Those complexing reagents and any complexed metals are then removed.
The process involves the conjugation of the linker, such as an amine-reactive (or thiol-reactive) chelator, to the antibody. This reaction is optimized with respect to the molar ratio of the chelator to the antibody (usually exhibits a Gaussian distribution of about 1.0 to 3.0 molar ratio of the chelator to antibody). The resulting mixture is subject to tangential flow filtration (TFF) to remove excess chelator and achieve buffer exchange into the final buffer at the desired concentration. TFF is ideal for this step, because it is widely used in pharma and is readily scalable. Other factors taken into consideration for developing and optimizing such conjugates include conjugation time and temperature, antibody concentration, appropriate conjugation buffer, use of organic solvents (to solubilize the chelator if required), pH, and mixing, among others.
A challenge at this point is the comprehensive characterization of the conjugate. Characterizing antibodies on their own can be difficult, because they are such large molecules; it is even more challenging when the antibody is conjugated to a linker. It is necessary to characterize the whole molecule, as well as its individual components. Using liquid chromatography (LC)-mass spectrometry and other advanced analytical techniques may be necessary to precisely determine the molar chelator–antibody ratio.
The final step is the addition of the radioisotope to the linker. While this chemistry is not necessarily difficult, characterization can be complicated, including varying half-lives of the radioisotope used, generally from about an hour to a few days. In addition to physicochemical characterization, it is necessary to use radio detection equipment to determine the level of radioactivity.
In general, because the manufacturing process is multi-step and the product comprises three distinct components, — viz: the antibody, chelator, and radionuclide constituting the radioimmune conjugate— there are some manufacturing and regulatory complexities. The regulatory complexities are borne from the fact that one has to follow the regulatory guidelines for not only the GMP manufacturing of the antibody and antibody–chelator conjugate (drug intermediate) but also radionuclide manufacturing and regulations to afford the radioimmune conjugate (drug product) and handling facility.19 Other issues include sourcing and handling of the radioactive materials, obtaining the appropriate licenses, accessing skilled operators and specialized training, and managing waste.
An even bigger question that must ultimately be addressed by theranostics makers, according to Deitcher, is whether the drug should have the radioactive payload added by the pharmacist in the hospital or whether manufacturing should be done centrally, with the radioactive product then delivered to the hospital or clinic ready to administer. It is a complex question, and the answer often depends on the isotope and its half-life. Most companies are currently attempting to use isotopes that allow for central manufacturing.
There is also the question about how theranostics are developed: linking a radionuclide to an antibody that is known to bind to a particular tumor cell or looking at which cancers are not yet benefitting from recent innovations and seeking to find antibodies that can deliver alpha-emitting radioisotopes.
Streamlining Theranostics Manufacturing at GBI12–18
GBI has been developing and manufacturing a wide range of bioconjugates for more than two decades. Many projects have involved radioisotopes, fluorescent dyes, and other payloads that are suitable for theranostic applications (Table 1). We have experience in working with both biomolecules and small molecules and have a deep understanding of the interface between organic chemistry and protein chemistry, including what is required to characterize bioconjugates. Furthermore, we have the expertise and knowhow to perform conjugation process optimization and scale-up and GMP manufacturing with process economics and compliance considerations to generate clinical, therapeutic-grade bioconjugates from lab to commercial scale. This includes the utilization of systems such as TFF, Mettler-Toledo Easy Max advanced synthesis workstation to precisely control conjugation and chemical processes, and size-exclusion chromatography, among others.
Table 1. Selected Radioimmune Conjugates Manufactured by GBI.
*Denotes projects including process development (PD), scale-up, and cGMP manufacturing
For theranostics, a key aspect of process development is the optimization of the molar ratio of payload, linker, and vector. Knowledge of which chelators are suitable for diagnostic and therapeutic applications is also essential. For poorly water-soluble linkers and payloads, the ability to balance the use and amount of organic solvents and reagents to ensure that the antibody vector remains intact is crucial, as proteins may aggregate under such conditions. In addition, some antibodies are more fragile than others, and the propensity to aggregate or degrade may increase once they are covalently linked to small molecules.
For each new project, GBI applies the learnings from hundreds of previous and ongoing projects (including complex biologics such as bioconjugates, monoclonal and polyclonal antibodies, Fc-fusion proteins, conjugate vaccines, bispecific antibodies and proteins, cytokines, enzymes, and other recombinant proteins) to the design of streamlined optimization studies. In addition, we are a single-source provider, and therefore manage the entire supply chain for our customers, viz: GMP cell banking, process development, scale-up and GMP manufacturing of the “naked” antibody (or recombinant protein), conjugation of the antibody onto the payload, and aseptic fill and finish.
Furthermore, GBI also manages other activities, such as IND-enabling activities, including characterization of the antibody–chelator conjugate (drug intermediates), stability studies with a range of fit-for-purpose buffers, and creation of reference standards, among others. Since GBI’s production site is not an organic synthetic chemistry facility, we work closely with partners that have the necessary expertise and licenses to produce chelators and small molecule payloads, including radionuclides.
It is also worth noting that, for antibody–chelator conjugates leveraging CHX-A” DTPA as the linker, GBI has developed a proprietary analytical method for quantification of this chelator, which can be quite challenging due to its complex structure. We have shown that the results obtained with this fluorescent spectroscopy method correlate well with the results obtained using LC-MS, while results are available immediately rather than taking weeks to receive data from the contract analytical lab. This proprietary rapid analytical technique contributes to our ability to accelerate optimization development to achieve the appropriate molar ratio of the antibody–chelator conjugate, which is particularly important for theranostic candidates that have received Fast Track, Breakthrough Therapy, or Accelerated Approval designations.
Ultimately, GBI’s experience and awareness of the unique development and manufacturing requirements associated with bioconjugates, combined with our ability to analyze antibodies and linkers to determine the best approach for delivering payloads, including radioisotopes, is significantly valuable to customers.
Conclusion
Theranostics show significant promise for complementing and supplementing immunotherapies as personalized cancer treatments. As high-value and complex products comprising vectors, linkers, and payloads, specialized expertise in bioconjugation is essential to developing and manufacturing optimal candidates that can provide highly targeted diagnostic and therapeutic benefits. Working with a contract development and manufacturing organization such as GBI with demonstrated experience in bioconjugation from the lab to the clinic and commercialization ensures that new safe, and effective theranostic products reach the market in an accelerated and cost-effective manner.
References
Wilson, Damien Jonas. “What is Theranostics?” News Medical Life Sciences. 13 Nov. 2018.
Qorri, Bessi, Alexandria DeCarlo, Matthew Mellon, and Myron R. Szewczuk. “Chapter 20 – Drug delivery systems in cancer therapy.” Drug Delivery Devices and Therapeutic Systems: Developments in Biomedical Engineering and Bioelectronics. Pages 423–454.
Sesay M. and C. Fang. “Early Phase Development Considerations of Antibody-Payload Conjugates.” Presentation at the World ADC Conference. San Diego, California. 18 Nov. 2018.
Antibody–drug conjugates (ADCs) are highly effective in therapeutic applications, particularly as anticancer agents. Technologies for linking small molecule payloads to biomolecules have steadily evolved since the field’s inception, resulting in continuous improvement in safety and performance. Manufacturing these multi-component therapies is challenging, however, given the three different elements––antibody, linker, and payload––require specialized capabilities. Integrating development and production activities within a single outsourcing partner can dramatically simplify ADC projects and accelerate timelines.
Growing Applications for Bioconjugates
Bioconjugates comprise a biomolecule, such as an antibody, protein, or peptide, linked to a payload, which is typically a small molecule active pharmaceutical ingredient (API) with a specific therapeutic activity. Proteins conjugated to small molecules find use in diagnostic applications, and various types of bioconjugates are used by researchers to investigate disease mechanisms and other biomolecular pathways.1
Antibody–drug conjugates (ADCs) are the most well-known bioconjugates and have been shown to be highly effective targeted therapies, particularly in the oncology space. The U.S. Food and Drug Administration (FDA) approved eight ADCs between 2019 and 2022. Furthermore, the number of ADCs entering phase I clinical trials in 2022 was 90% higher than in 2021, while the total number of clinical studies investigating ADCs that were initiated in 2022 was 35% higher than in the previous year.2
The global market for ADCs is valued at approximately $9 billion in 2023 and is estimated to be expanding at a compound annual growth rate around 11%.3,4 In June 2023, 11 FDA-approved ADCs were on the market.1 This strong growth is attributable to the increased effectiveness of later-generation ADCs, which have significantly improved stability and pharmacokinetic properties.
Most approved and candidate ADCs are anticancer therapies, with approximately one-fifth targeting the oncoproteins HER2 and TROP2. Other targets being explored include BCMA, CD19, CD22, CD30, CD33, Fra, and TF, among many others.2 Over 30 different linker chemistries and more than 60 different payloads have been employed in clinical candidates, although approximately half of clinical ADCs have leveraged tubulin inhibitors, which disrupt the cytoskeleton in targeted cells, leading to cell death.
Advances continue to be made in linker chemistry, payload design, and antibody engineering. Examples include immune-stimulating antibody conjugates (ISACs) that activate immune responses and radioactive and cytotoxic payloads. Payloads, such as kinase inhibitors, are being investigated to determine if targeted administration will improve the therapeutic index. In addition, researchers and biopharmaceutical companies are showing growing interest in the use of other biomolecules, most notably peptides, that can penetrate solid tumors more efficiently than antibodies. Single-chain antibodies, antibody fragments, bispecifics, and other alternatives are also being explored. ADCs are being evaluated in the clinic as combination therapies with other chemotherapeutic agents.
Evolving Bioconjugation Solutions
The first ADC was approved in 2000. Mylotarg (Pfizer’s gemtuzumab ozogamicin) leveraged N-acylhydrazone linker technology, which unfortunately proved to be unstable and resulted in severe liver toxicity, leading to a withdrawal of the drug in 2010. However, it received approval again in 2017 at a lower dosage administered over a longer timeframe, which reduced toxicity.
Challenges with early linker technology drove significant efforts to identify improved alternatives, and new approaches were introduced in 2004–2005. In general, the linker technologies used in first-generation ADCs provided no control over the number of payloads conjugated to the antibody, leading to unsuitable heterogeneity of drug-to-antibody ratios (DARs).5 Release and reattachment of payloads at different locations and conjugation to many areas of the antibody, including the binding region, led to reduced efficacy and in some cases release of the payload in non-target tissues.
Second-generation ADCs benefited from site-specific conjugation (controlled linker location and homogeneous DAR values) and linkers that only release their payload when exposed to certain conditions in the target cell (e.g., a certain pH, high concentration of certain enzyme).5 Such cleavable linkers were an improvement over early non-cleavable linkers that required degradation of the targeting agent for the payload to be released.
Based on prior experience with first- and second-generation ADCs, third-generation ADCs are built on advances with dual-cleavage linkers for more specific payload release and linkers that can bind to multiple payloads for greater potency, in combination with solutions that better accommodate hydrophobic payloads for improved solubility and bioavailability.5 An example is the use of liposomes and branch chain linkers that can be loaded with multiple payload molecules.
Overcoming Supply Chain Challenges with Integration
ADC developers relying on a fragmented supply chain face a range of challenges associated with the intricacies of vendor management. With multiple suppliers to oversee, each specializing in a unique ADC component (antibody, linker, and payload), companies frequently wrestle with harmonizing quality controls, synchronizing timelines, and ensuring efficient communication among all entities. The absence of an integrated service also exposes developers to potential inconsistencies in product quality. As each vendor enforces its distinct set of quality parameters, discrepancies can emerge, affecting the final ADC product’s potency and safety. Moreover, aligning timelines among varied suppliers can evolve into a logistical conundrum, which may culminate in unforeseen production delays. The transportation and storage of ADC components pose another layer of complexity. Developers must navigate the logistical hurdles of receiving materials from different geographical locations, each presenting unique bottlenecks. The diverse storage prerequisites for distinct components, ranging from specific temperature controls to unique handling protocols, can further complicate the process, requiring heightened vigilance and resource allocation.
Given these complexities, sourcing raw materials for ADC production can be more challenging than procuring material for conventional antibodies. ADCs –– constituted of biological, small molecule components –– and a linker, necessitate that each of these three elements be manufactured in compliance with cGMP standards. All three components must then be concurrently delivered to the site designated for bioconjugation. Recognizing these challenges, manufacturers have made concerted efforts to consolidate as many relevant activities as feasible, either in-house or through alliances with contract development and manufacturing organizations (CDMOs) that offer comprehensive support for ADC production.
Integration of drug intermediate (antibody, linker, and payload) manufacturing within a single provider, coupled with drug substance and drug product manufacturing, streamlines project management, rendering the establishment of ADC production timelines more straightforward. Moreover, these timelines are typically shorter, and there is a heightened probability of adhering to them. Crucially, every element is fabricated under a unified quality management system, promoting efficient communication between development and production teams.
Samsung Biologics aims to offer fully integrated capabilities for ADC development and manufacturing. Currently, the company has expertise in antibody engineering, process development, and large-scale manufacturing of antibodies. The process development group is ramping up its capabilities in bioconjugation and adding experienced personnel to its expanding team.
Samsung Biologics will add the capability to expand its drug product manufacturing to include cytotoxins. This move is not only aimed at achieving full integration, but also at circumventing the challenges associated with accessing fill/finish services for cytotoxics and shipping these materials globally. The company is currently evaluating whether small molecule manufacturing will be established internally, via an acquisition, or through a licensing arrangement with another company.
Customers can expect that, regardless of the chosen route, Samsung Biologics will establish integrated capabilities and the necessary expertise for ADC manufacturing in the near future. Indeed, the company is a relatively recent upstart but is already one of the largest manufacturers of monoclonal antibodies in the world. The approach to integrated ADC manufacturing will be similar––and significant. The company is very adept at constructing facilities and reducing timelines. Samsung Biologics expects to be a major player in the ADC market moving forward.
Enabling Bioconjugation through Appropriate Facility Design
In addition to aseptic manufacturing, which is required for all biologics, the cytotoxic nature of most ADCs requires the establishment of an environment suitable for handling highly potent and cytotoxic molecules. Not only must personnel be isolated from the process, but the process must also be isolated from the personnel. Effective containment for highly potent compounds involves rigorous control of the flow of personnel, materials, and room air.
Multiple mechanical seals are employed when the conjugation vessel is operational to prevent any release of material to the surrounding environment. “Air curtains” are used as shields for certain steps. The air turnover rate in a room for processing highly potent compounds must be extremely high (somewhere between 25 and 50 air changes per hour). For certain molecules and operations, personnel may be required to wear special respirators or air masks. Gloveboxes are typically used when preparing solutions of the cytotoxic compound to prevent release of even very small quantities of cytotoxic powder into the environment. The facility must be equipped with HEPA and carbon filters to remove even trace amounts of cytotoxins in the air and prevent their exhaustion to the environment.
Unlike traditional biologic processes, waste generated during the processing of highly potent compounds must be incinerated. That includes liquids from chromatography columns and tangential-flow filtration (TFF) systems (up to thousands of liters) and solids.
Changeover from one bioconjugation process to another when cytotoxic payloads are involved is more challenging as well. In addition to monitoring for microbial contamination, it is necessary to determine whether any residual cytotoxic materials are present. That requires analysis using liquid chromatography-mass spectrometry (LC-MS) to detect minute levels of toxins.
A truly integrated ADC service provider should have equipment that will be dedicated to certain cytotoxic payloads widely used in ADCs (e.g., tubulin inhibitors). It is also expected that, where it is possible to limit the quantity of organic cosolvent required to solubilize the cytotoxic payload before conjugation, such as for less hydrophobic compounds, single-use systems will be employed. To meet the required co-solvent level, ADC candidates must be produced in stainless steel or borosilicate glass-lined reaction vessels simply because of the level of co-solvent required.
Importance of the Right Analytical Support
Given that ADCs involve a biologic large molecule, a small molecule, and linker components that may be enzymes, peptides, or polymers, a wide range of analytical capabilities are needed to support process development, process monitoring, and product release.
For product release, typical methods are required to analyze the naked antibody, but others are also needed to evaluate the conjugated antibody (e.g., DAR, sites of conjugation). It is also necessary to confirm that no free payload molecules are present. Separate methods are needed to confirm the identity and purity of the payload and the linker before their attachment and to confirm proper attachment to one another. Finally, at least one biological, cell-based assay is needed as well. All told, approximately 15 different analytical methods are required to release an ADC drug substance.
Overcoming Market Hurdles
The ADC field continues to advance at a rapid pace, with scientific knowledge expanding exponentially as more candidates progress through the development cycle. More information is being gained on how ADCs harness and activate the immune system and kill cancer cells. With this knowledge, the design of targeting agents is improving, and new payloads and linkers will enable treatment of a wider range of oncology indications. New companion diagnostics designed around the physiology of the therapeutic indication will increase the patient response rate. ADCs are designable therapeutics where our prior experience will increase the probability of success for the next generation of ADCs. The future is very exciting, and Samsung Biologics, given its unparalleled track record of success in biologics development and manufacturing services, is well poised to play a major role in bringing these novel treatments to patients safely and as cost-effectively as possible.
Antibody–drug conjugates are highly complex, and their manufacture involves multiple and disparate technologies. Most biopharmaceutical companies, therefore, rely on contract service providers. Working with different suppliers for each part of the process can potentially add risks, time and cost to an ADC production program. The PROVEO™ Alliance overcomes these difficulties by offering streamlined support from antibody production through conjugation and fill-finish to labeling and packaging.
Positive ADC Outcomes Driving Market Growth
Antibody-drug conjugates (ADCs) are next-generation antibody therapies that provide targeted delivery of cytotoxic anti-cancer agents to cancer cells. They comprise an antibody and a cytotoxic payload that are conjugated via a linker. By avoiding systemic delivery and attacking the cancer cells directly, ADCs offer increased efficacy with reduced side effects. As technology has advanced, second- and third-generation ADCs have become safer and even more precisely targeted.
There are currently six marketed ADCs and approximately 250 ADC candidates under development.1 Of those, nearly 40% are undergoing clinical studies, with over half targeting solid tumors. ADCs account for approximately 20% of the clinical pipeline of antibodies for cancer.2 With 11 additional drugs in late-stage clinical development, double-digit approvals are expected in the next few years.3
Significant R&D effort is focused on expanding the types of conjugated payloads, targeted indications and treatment protocols, particularly their use in combination therapies.4 In addition, 40 trials are underway involving ADC/checkpoint inhibitor combination therapies for the treatment of various cancers. ADCs are also being developed with payloads other than small molecules, such as proteins, enzymes and Fab fragments, the latter of which generates bispecific antibodies.
The value of the global market for ADCs is estimated to be expanding at a compound annual growth rate in excess of 20% and expected to reach $15 billion by 2030.1 Notably, more than $5 billion has been invested in this ADC sector, and partnership activity has increased at an annual rate of 30%.1
Combining the strengths and expertise of three industry leaders into one simplified ADC solution, PROVEO delivers streamlined support from antibody production through conjugation and fill-finish to labeling and packaging, all tailored to each client.
Complex Products and Manufacturing Processes
Monoclonal antibodies used in ADCs should be designed for manufacturability at scale.5 They need to be robust, stable biomolecules that can withstand the further processing conditions involved in ADC production and contain the appropriate sites for conjugation to the cytotoxic payload via the desired linker chemistry. The drug (payload)–antibody ratio (DAR) and sites of conjugation must be carefully controlled and verified, as they directly impact the potency and efficacy of the ADC. Undesired payload binding and other modifications of the antibody can potentially lead to reduced stability (i.e., aggregation), reduced efficacy and immunogenicity and other adverse patient reactions. ADC purification often requires unique equipment and capabilities.
ADC drug substance manufacturing needs to balance bioburden-controlled activities while ensuring protection of operators and the environment from exposure to the highly potent payloads. Achieving these two goals requires conflicting control of air flows and air pressure in the facility. Extensive use of isolators in combination with unique facility designs is required to protect the product components, operators and the environment. As such, facilities for the production of ADCs require high capital investment and extensive operator training.5
Manufacturers must have capabilities in cell culture and synthetic chemistry and a deep understanding of conjugation chemistry, which must be highly controlled to ensure proper site selectivity and prevention of aggregation.6 Fill-finish capabilities, including lyophilization, are also necessary. Furthermore, because ADCs are highly complex, structurally heterogeneous and often contain not just a single product, but many product-related species, analytical expertise that bridges biology and chemistry is absolutely essential to ADC characterization and control.7
Reliance on Contract Manufacturers
The complexity of ADC development and manufacturing has led many biopharmaceutical companies to turn to contract development and manufacturing organizations (CDMOs) for assistance with their ADC projects. According to one estimate, at least 70% of ADC manufacturing is outsourced, and this level will increase, owing to the fact that many third-generation ADCs are being developed by small biotech and specialty pharma firms that require extensive support and access to the specialized expertise and facilities required for ADC production.5
By offering the services of specialists across multiple teams within a single, global service backed by years of experience, PROVEO helps companies save time, cost and resources across all aspects of the ADC production cycle.
Integrated Solutions Facilitate Accelerated Development
Only a few CDMOs have the capability to perform all of the steps involved in ADC manufacturing, including production of antibodies, linkers and payloads, conjugation and fill-finish. Integrated service offerings provide several advantages, most notably reduced time to market due to elimination of multiple suppliers (antibody, linker, payload and ADC producers, as well as potential separate fill-finish, packaging and distribution service providers) and to transfer product from one service provider to another.6 Most importantly, potential scheduling snafus are avoided. Working with an integrated ADC CDMO also reduces and de-risks supply chain complexity while freeing up management time and resources.
PROVEO™
Combining the strengths and expertise of three industry leaders into one simplified ADC solution, PROVEO delivers streamlined support from antibody production through conjugation and fill-finish to labeling and packaging, all tailored to each client. The service is designed to provide significant efficiency gains in the ADC manufacturing process by bringing together specialized companies that are globally qualified and able to provide product development and manufacturing support, creating value through integrated project and supply chain management.
PROVEO is a solution provided by AGC Biologics, Cerbios and Oncotec Pharma Produktion GmbH to simplify the complexity of ADC outsourcing. All three companies are well-established, global suppliers that work together to reduce the time, cost and resources required for ADC manufacturing, giving customers multiple development and manufacturing options.
PROVEO supports the entire ADC supply chain: the development of a microbial or mammalian cell line, as well as production and purification processes to deliver the purified binding protein for the ADC; design of appropriate manufacturing processes for the payload, linker and bioconjugation step with cGMP production of the ADC drug substance; and sterile filling and labeling of the drug product.
“Safe” early transfer steps were identified and supported by a transfer framework that enables fast development of optimized ADC processes and products. Across all sites, we use harmonized basic analytical methods and share the analytical methods specific to each phase of a project. As a result, we are able to compare results and reduce or avoid the need for method transfer. In addition, harmonization of quality assurance across the whole supply chain is achieved through a shared quality agreement and cross-auditing, making it possible to guarantee a high level of QA standards throughout the entire manufacturing process from monoclonal antibody (mAb) to packaged ADC product.
PROVEO also employs a fully integrated project management system across the supply chain with a single program manager that works with project managers at each site. This approach allows for seamless transitions across the network and enables complete integration of development and manufacturing efforts. As a result, we can provide risk-free timeline compression, reducing the time it takes from DNA to fill-finish from 30 months for the traditional supply chain with four separate providers to 20 months.
Antibody Manufacturing Expertise
AGC Biologics is one of the largest global biologics CDMOs specializing in the clinical and commercial development of therapeutic proteins, with a 15+ year track record of technical success in development and cGMP manufacturing. A leader in the implementation of innovative technologies and solutions that accelerate time to market, AGC has an agile, entrepreneurial culture and a commitment to cultivating strong partnerships that enable client success. AGC Biologics also has experience successfully transferring processes and technologies between sites to facilitate scale-up or market expansion
Monoclonal antibodies are produced at AGC’s FDA- and EMA-approved sites in Copenhagen, Denmark and Seattle, Washington using the CHEF1® proprietary expression technology platform with four commercial products in the market, as well as other available expression systems. Mammalian capacities range from 100 to 12,000 L in single-use and stainless-steel equipment, and mAb manufacturing is supported by experts in process, analytical and drug substance/drug product formulation development, including stability testing and bioassays.
Payload and Conjugation Expertise
Cerbios has over 40 years of experience in the development of processes for the production of APIs and 25 years of experience handling highly potent compounds, with products marketed in over 60 countries. Payload and linker production and ADC conjugation are performed at Cerbios’ FDA-, PMDA- and SwissMedic-approved facility in Lugano, Switzerland. The facility is designed to handle highly potent payloads to category 4 and has dedicated conjugation units. Analytical experts provide process characterization, stability testing, product release testing and other QC/QA support on site, while regulatory experts assist clients with preparation for filing of INDs and NDAs.
The Cerbios site includes three cGMP payload and linker production units supporting clinical and commercial batch sizes from 10 to 30 kg. Specialized equipment available for payload and linker production and conjugation processes include Biotage and PLC chromatography units, a photoreaction unit and continuous flow chemistry solutions, all benefiting from modular containment. Conjugation is performed in two cGMP production units at batch sizes from 5 to 200 L, leveraging purification technologies such as single-use bio-chromatography and tangential-flow filtration, also in modular containment.
Fill-Finish Expertise
Oncotec has been manufacturing sterile products for oncological indications since 1999, providing contract manufacturing services for highly potent substances to more than 20 companies. The plant in Dessau, Germany has been successfully inspected by numerous regulatory authorities, including the FDA, ANVISA, PMDA, FDA Saudi-Arabia and the Turkish, Libyan and Russian MoHs.
The final formulation, sterile filling, packaging and labeling of final ADC drug products takes place at Oncotec. Both small- and large-scale aseptic filing lines with lyophilization and vial-washing capabilities are available for the production of highly potent ADCs. Vial sizes from 2 to 200 mL are supported. The freeze dryers have capacities of 0.6 and 30 m². The filling machine is robotic, and filling is achieved using peristaltic pumps with a line speed of 5000 vials/hour. The system can handle products formulated in solvents. There is also the possibility to fill ADCs into disposable bags.
Case Studies Underscore PROVEO Alliance Benefits
Given a mAb sequence, PROVEO developed an initial lab-scale process and limited analytics and then established a stable, monoclonal CHO cell line using the CHEF1 platform (3.2 g/L). Upstream and downstream processes and analytics were developed based on the existing platform. The yield was then further improved by 25%, with acidic species reduced during upstream process development. The production process was successfully scaled, providing GMP material just 12 months after initiation of the project.
A medicinal chemistry process for milligram-scale production of a payload did not afford any robustness or reproducibility, and the product had an insufficient quality (90%) and contained unidentified impurities. Using a quality-by-design (QbD) approach and following Q11 rules, process and analytical development efforts were pursued. A process controls strategy was then developed in collaboration with the customer. The resulting process was robust and reproducible and afforded a much higher yield at significantly reduced COGS. Both the synthesis and HPLC purification steps were scaled successfully. Several cGMP lots were completed at the hundred-gram scale and the analytical methods were validated for the late clinical-phase investigational drug.
For an ADC product, a laboratory-scale process using novel, site-specific bioconjugation technology and with limited established analytical methods needed to be scaled up for cGMP manufacturing. A QbD-like approach was used to design an optimized (time, yield and COGS), robust, reproducible process that generated the ADC drug product in a form that enabled integration of pre-formulation into the sterile fill-finish process. Analytics were also developed for both in-process control and GMP release. A GMP lot of the ADC drug substance was produced for use in a phase I clinical study.
A laboratory-scale fill-finish process that did not include lyophilization and had limited established analytical methods required scale-up and the addition of a lyophilization step. A formulation compatible with freeze drying was developed in collaboration with the client, and an efficient lyophilization cycle was identified following completion of a designed experiments study. The optimized process was first scaled to the pilot plant and then to GMP manufacturing, with GMP batches of the ADC drug product successfully produced.
Getting Medicines to Patients Sooner
By offering the services of specialists across multiple teams within a single, global service backed by years of experience, PROVEO helps companies save time, cost and resources across all aspects of the ADC production cycle.
References
Wagh, Anil, Hantian Song, Ming Zeng, Li Tao and Tapan K. Das. “Challenges and new frontiers in analytical characterization of antibody-drug conjugates.” MAbs. 10: 222–243 (2018).
Harper, Rachel. “Antibody drug conjugates market to be worth $15bn by 2030.” European Pharmaceutical Review. 30 Aug. 2019. Web.
“Antibody Drug Conjugates in Cancer Drug Development.” IQVIA. 2018. Web.
Hofland, Peter. “Experts Forecasts CMOs to Benefit from Double Digit Approvals of ADCs.” ADC Review. 23 Oct. 2018. Web.
Johnson, Charlie. “The Evolving Market for Antibody-drug Conjugates: How Widening Applications and Manufacturing Improvements help Meet Growing Demand.” ADC Review. 1 Apr. 2019. Web.
Scanian, Claire et al. “Antibody-drug Conjugates: Manufacturing Challenges and Trends.” ADC Directory. 15 Jan. 2019. Web.
Sharma, Vivek. “CPhI Annual Report 2018: ADCs Growth Driven by Lack of In-House Facilities, Oncology and Integrated CDMOs.” Pharmaceutical Outsourcing. 10 Oct. 2018. Web.
Originally published on PharmasAlmanac.com on December 6, 2019